- Benjamin G. Domb, M.D.a,
 ,,
,, - Marc J. Philippon, M.D.c,
- Brian D. Giordano, M.D.b
- a Hinsdale Orthopaedics, Hinsdale, Illinois, U.S.A.
- b University of Rochester, Rochester, New York, U.S.A.
- c The Steadman Clinic, Vail, Colorado, U.S.A.
- http://dx.doi.org/10.1016/j.arthro.2012.04.057, How to Cite or Link Using DOI
- Permissions & Reprints

Purpose
The purpose of this systematic review was to critically evaluate the available literature exploring the role of the hip joint capsule in the normal state (stable) and pathologic states (instability or stiffness). Furthermore, we examined the various ways that arthroscopic hip surgeons address the capsule intraoperatively: (1) capsulotomy or capsulectomy without closure, (2) capsulotomy with closure, and (3) capsular plication.
Methods
Two independent reviewers (B.D.G. and B.G.D.) performed a systematic review of the literature using PubMed and the reference lists of related articles by means of defined search terms. Relevant studies were included if these criteria were met: (1) written in English, (2) Levels of Evidence I to V, (3) focus on capsule and its role in hip stability, and (4) human studies and reviews. Articles were excluded if they evaluated (1) total hip arthroplasty constructs using bony procedures or prosthetic revision, (2) developmental dysplasia of the hip where reorientation osteotomies were used, (3) syndromic instability, and (4) traumatic instability with associated bony injury.
Results
By use of the search method described, 5,085 publications were reviewed, of which 47 met appropriate criteria for inclusion in this review. Within this selection group, there were multiple publications that specifically addressed more than 1 of the inclusion criteria. Relevant literature was organized into the following areas: (1) capsular anatomy, biomechanics, and physiology; (2) the role of the capsule in total hip arthroplasty stability; (3) the role of the capsule in native hip stability; and (4) atraumatic instability and capsulorrhaphy.
Conclusions
As the capsuloligamentous stabilizers of the hip continue to be studied, and their role defined, arthroscopic hip surgeons should become facile with arthroscopic repair or plication techniques to restore proper capsular integrity and tension when indicated.
Level of Evidence
Level IV, systematic review.
Hip joint stability is a marriage of complementary functions provided by static and dynamic stabilizers. In a normal state, the bony articulation between the femoral head and quasi-hemispheric acetabulum provides inherent stability to the hip. The congruence of the joint is further optimized by normal proximal femoral and acetabular offset, coverage, inclination, and version.1 and 2 The fibrous hip joint capsule is intimately related to a confluence of 4 capsular ligaments and expansions that provide static constraint to the joint throughout a wide variety of physiological motions (iliofemoral, pubofemoral, and ischiofemoral ligaments and zona orbicularis). Biomechanical studies have suggested that these ligaments work in concert with other periarticular static soft-tissue stabilizers, such as the acetabular labrum, transverse acetabular ligament, pulvinar, ligamentum teres, and iliocapsularis muscle.2, 3, 4, 5, 6 and 7 Because of their spiral configuration, the leash-like fibers of the zona orbicularis and capsular ligaments tighten in a “screw-home” mechanism during terminal extension and external rotation, imparting further stability to the joint.3, 6 and 8 In addition, neuromuscular factors and dynamic stabilizers such as the iliopsoas, rectus femoris, and abductor complex also contribute to the overall maintenance of proper joint kinematics and force-coupled compression that enhance hip joint stability.2, 5 and 6
Instability has been recognized as a pathologic condition that can affect the function of the hip in a number of ways.5, 6 and 9 The continuum of hip instability is typically categorized into traumatic or atraumatic etiologies based on mechanism and clinical presentation.6 Traumatic hip instability is usually associated with a distinct event such as high-energy dislocation, with or without concomitant bony injury. However, lower-energy injuries may also result in a subtle traumatic subluxation episode that is less obvious. Atraumatic instability of the hip is a poorly recognized clinical entity that is emerging in the orthopaedic literature as a significant cause of functional impairment in the young patient.5 and 6 In the senior author’s series on revision hip arthroscopy, 35% of patients were found to have undiagnosed atraumatic instability.10 Usually, this occurs as the result of repetitive motion patterns that lead to microinstability, and it can ultimately result in progressive labral and chondral injury.
Restoration or reconstruction of native anatomic relations is a fundamental tenet of modern athletic medicine. Regardless of the joint, most arthroscopic surgeons strive to restore normal anatomy with the goal of optimizing native joint physiology and kinematics. Arthroscopically assisted anterior cruciate ligament (ACL) reconstruction has received considerable attention in recent years for its transition to more anatomically focused reconstruction techniques.11 Bedi and Altchek12 emphasize the importance of this dogmatic shift in their concise review on anatomic ACL reconstruction. Furthermore, in an editorial commenting on this publication, Lubowitz and Poehling13 state that they “continue to contend that anatomic placement of ACL reconstruction grafts is the critical key to successful outcome.” Moreover, “This isn’t unique to ACL reconstruction.”
Restoration of normal hip morphology, as well as the physiological “sealing mechanism” of the acetabular labrum, has been a primary goal of hip surgeons since Ganz et al.14 developed the concept of femoroacetabular impingement (FAI) and proposed a novel surgical approach to address the underlying pathoanatomy.15 and 16 In open FAI surgery, as described by Ganz et al., the hip joint capsule is typically breached with a Z-cut that is usually repaired at the conclusion of the case. In contrast, arthroscopic FAI management techniques have placed less emphasis on restoring the integrity of the hip joint capsule. Instead, most rely on extended capsulotomies or even focal capsulectomies to achieve the same goals as open hip surgery.17 and 18 Despite biomechanical evidence highlighting the role of the hip joint capsule in maintaining functional stability, capsulotomies and capsulectomies continue to be performed with great frequency, with little regard for potential consequences. Some arthroscopic hip surgeons have postulated that an aggressive capsulotomy actually has the potential to be therapeutic in the setting of preoperative stiffness.19, 20, 21, 22, 23 and 24
Unfortunately, with the growing popularity of arthroscopic hip surgery, iatrogenic instability from excessive capsulotomy/capsulectomy is becoming a growing concern.25, 26 and 27 As arthroscopic hip surgeons continue to gain a more firm understanding of the pathophysiology of hip instability, greater emphasis is being placed on preserving the capsule. Some authors have begun to advocate complete or partial capsular closure to restore proper capsular stability at the termination of the case.18 Others have reported on capsular volume reduction techniques for atraumatic hip instability, such as thermal capsulorrhaphy or suture plication.28, 29, 30 and 31
The purpose of this study was to critically evaluate the existing evidence in support of (1) capsulotomy or capsulectomy without closure, (2) capsulotomy with closure, and (3) capsular plication. In addition, literature on the role of the capsule in stability versus stiffness is reviewed.
Methods
Two independent reviewers (B.D.G. and B.G.D.) performed an exhaustive search of PubMed for articles that contained at least 1 of the following search terms: hip capsule, hip capsular, hip instability, hip stability, hip plication, hip capsulorrhaphy, atraumatic hip instability, hip capsulectomy, and hip capsule repair. The search included articles published from January 1930 to October 2011. In addition, reference lists from the relevant articles were retrieved to identify any additional studies of interest. Full publications were obtained for relevant studies that had potential to meet our inclusion criteria: (1) written in English, (2) Levels of Evidence I to V, (3) focus on capsule and its role in hip stability, and (4) human studies and reviews. Articles were excluded if they evaluated stability in total hip arthroplasty (THA) constructs that emphasized bony procedures or prosthetic revision, developmental dysplasia of the hip where reorientation osteotomies were used, or syndromic instability (e.g., Down syndrome, arthrogryposis, or neuromuscular) or if they reported on traumatic instability where there were associated bony abnormalities requiring treatment.
Results
By use of the search method described, 5,085 publications were reviewed by B.D.G. and B.G.D. Forty-seven articles ultimately met appropriate criteria for inclusion in this review. Within this selection group, there were multiple publications that specifically addressed more than 1 of the inclusion criteria. This is reflected in the breakdown of literature by topic and overlapping inclusion of relevant articles. Ten articles in this review directly addressed the biomechanical importance of the hip capsule.2, 3, 4, 8, 20, 32, 33, 34, 35 and 36 Ten relevant studies discussed the critical role of the hip capsule in maintaining total hip construct stability.4, 37, 38, 39, 40, 41, 42, 43, 44 and 45 Seven publications emphasized the role of the native hip capsule in hip stability.3, 9, 18, 25, 26, 27 and 46 Six articles addressed capsulotomy/capsulectomy as a viable treatment option for hip joint stiffness.19, 20, 21, 22, 23 and 24 Three contemporary reviews have advocated and described various technical approaches for capsular repair after arthroscopic instability or FAI surgery.9, 18 and 46 In our search we uncovered 8 review publications that mentioned arthroscopic thermal capsulorrhaphy.5, 6, 9, 28, 30, 31, 47 and 48 The same 8 articles also mentioned arthroscopic suture capsulorrhaphy as an established method to treat hip instability. There were 12 total clinical reports that discussed the use of arthroscopic or open capsulorrhaphy (thermal or suture) to treat hip instability.6, 10, 49, 50, 51, 52, 53, 54, 55, 56, 57 and 58 These were all case reports or small case series.
Discussion
Capsular Anatomy, Biomechanics, and Physiology
Hip arthroscopists routinely use capsulotomies and capsulectomies to address chondral-labral pathology or areas of pathologic bony conflict. Violation of capsuloligamentous structures in this process is often unavoidable. Usually, these capsular cuts are left unrepaired with unclear significance to the stability of the joint. Favorable short-term and midterm outcomes have been reported using this technique to address symptomatic acetabular labral tears, FAI, and other associated hip pathology.10, 15, 17, 18, 19, 59, 60 and 61 Although early success rates are uniformly high, there remains potential for improvement. Longer-term follow-up shows a slow decline in outcome scores, without a clear mechanism in many cases. Some series have even shown that a significant number of patients will ultimately require conversion to THA (12% to 28%).61, 62 and 63 Even more concerning is the fact that rare cases of postoperative subluxation and dislocation have been reported after arthroscopic hip surgery.25, 26 and 27 These sobering reminders highlight the need for ongoing technical improvements that allow intra-articular pathology to be sufficiently addressed while avoiding excessive attenuation of the capsuloligamentous stabilizers.25, 26 and 27
Although the hip is an inherently stable joint by virtue of its bony geometry, static and dynamic soft-tissue stabilizers play a considerable role in maintaining joint congruity throughout a physiological and supraphysiological range of motion. The anatomy, function, and physiology of the fibrous hip capsule have been extensively studied. 2, 3, 6, 8, 9, 20, 33, 34, 35, 64, 65, 66 and 67 Table 1 further describes the various contributions of the capsuloligamentous stabilizers. Telleria and colleagues 35 recently published a comprehensive arthroscopic description of the capsuloligamentous structures that is of particular relevance to the hip arthroscopist. They showed that these structures could be consistently identified using specific anatomic landmarks within the central and peripheral compartments of the hip.
Table 1. Capsular Anatomy, Biomechanics, and Physiology
| Capsular Structure |
Anatomic Origin |
Anatomic Insertion |
Function |
Misc |
|
Iliofemoral Ligament (Y ligament of Bigelow)2, 3, 38, 39, 40, 43 and 44 |
Anteroinferior iliac spine |
Courses distally over the FH to the intertrochanteric line |
Tightens in “screw home” mechanism during extension/ER |
Strongest of the capsular ligaments |
|
Anterior/anteroinferior portion exhibits highest tangent structural stiffness |
||||
|
Resists anterior translation |
Higher modulus of elasticity, and ultimate strength |
|||
|
Stabilizes capsule anteriorly |
Significantly thicker in cross-section |
|||
|
Pubic portion of the acetabular rim |
Posterior intertrochanteric crest (inferior to the ischiofemoral ligament) |
Reinforces capsule inferiorly |
Between iliofemoral and pubofemoral ligament, there is a gap in the capsule of unclear significance that can be tightened to affect capsular volume reduction without plication |
|
|
Provides restraint to ER, hyperextension, hyperabduction |
||||
|
Ischial rim of the acetabulum |
Courses as 2 discreet bands in spiral configuration around posterior FN |
Restricts IR in flexion and extension |
Blends with zona orbicularis posteriorly |
|
|
Broad insertion at anterosuperior to posterosuperior base of the greater trochanter |
||||
|
Zona Orbicularis 8 |
Encircles entire femoral neck |
Acts as a locking ring around the femoral neck |
Also referred to as annular or arcuate ligament |
|
|
Function and anatomy debatable |
||||
|
Represents convergence of fibers from medial arm of the iliofemoral ligament and pubofemoral ligament |
Imparts stability in distraction |
Some transect for greater exposure during arthroscopic femoroplasty |
ER, external rotation; FH, femoral head; FN, femoral neck; IR, internal rotation.
Because of their spiral configuration, the leash-like fibers of the zona orbicularis and anterior capsular ligaments tighten in a screw-home mechanism during terminal extension and external rotation, further stabilizing the joint.6 As the hip moves into flexion, the fibers unwind and loosen, rendering the joint less stable. The screw-home mechanism of the hip joint capsule may, in fact, represent an evolutionary adaptation that occurred as humans transitioned from quadrupeds to bipeds.66 and 67 Anthropologic literature supports the contention that as humans began to walk upright, the hips were brought into relative extension, thus causing the capsular fibers to twist into a spiral pattern.
Role of Capsule in THA Stability
The hip joint capsule has been shown to significantly impact total hip construct stability in both biomechanical and clinical trials. 4, 37, 38, 39, 40, 41 and 42 Capsular integrity in THA con-structs may serve as a proxy for native hip states, and meaningful conclusions can be extracted from careful review of these data. Elkins et al. 4 studied the relative contribution of the hip capsule in THA stability and found that reducing the capsule to a thinner size, or creating capsular attachment defects, substantially compromised construct stability. However, they showed that even in the worst scenario of structural compromise, suture repair returned stability to within approximately 10% of baseline levels.
A number of clinical trials on dislocation after THA have focused on the posterior approach to the hip, as well as on the influence of capsular repair on construct stability. 38, 39, 40 and 41 Mihalko and Whiteside 36 found that meticulous posterior capsular repair, combined with repair of the short external rotators, resulted in a more normal deflection curve when compared with the normal state. Various techniques for repair or capsulorrhaphy have been proposed with a low incidence of postoperative dislocation (0.85% to 2.8%). 38, 39, 40, 41, 44 and 45 Prospective studies have shown statistically significant reductions in the rate of postoperative dislocation in patients who underwent THA with posterior capsulorrhaphy versus capsulotomy without closure (0% to 0.6% v 2.3% to 2.8% for posterior capsulorrhaphy v capsulotomy alone). 40 and 41 Recent retrospective comparative series also support the conclusion that patients who undergo THA without repair have a significantly higher rate of postoperative dislocation (4.8% to 6.38% v 0% to 0.7% for capsulectomy v repair). 37 and 39 In the setting of revision THA, the importance of capsular integrity appears to be even more profound (17% with posterior capsulectomy v 2.5% with posterior capsular repair). 38 In some cases of tumor resection, where extensive capsulectomy is necessary, restoration or repair of the native hip capsule is impossible. In such instances, capsular replacement has been proposed using Achilles allograft of synthetic mesh. 42 and 43
Role of Capsule in Native Hip Stability
Although studies on THA construct stability support routine capsular repair, less attention has been paid to the role of the capsule in arthroscopic hip surgery. The senior author and his colleagues recently studied the relative contributions of the acetabular labrum and iliofemoral ligament in hip stability.3 They used a cadaveric model that simulated typical capsulotomy incisions used during hip arthroscopy. They found that external rotation and anterior translation were both significantly increased when the iliofemoral ligament alone was sectioned and were further increased when both the labrum and iliofemoral ligament were sectioned in concert. Interestingly, repair of the labrum alone did not result in normalization of external rotation or anterior translation, but repair of the labrum in conjunction with repair of the iliofemoral ligament adequately restored these parameters to the native intact state. These findings underscore the notion that careful attention to the capsule is necessary when addressing symptomatic labral tears or regions of bony impingement arthroscopically. In addition, these findings seem to suggest that gaining access to areas of chondrolabral pathology or zones of cam deformity through large capsulotomies may result in a significant degree of supraphysiological motion, thus minimizing the biomechanical advantage of performing arthroscopic labral repair.
Anterosuperior capsulotomy and capsulectomy have become commonly used in hip arthroscopy to address symptomatic FAI.15, 17, 18, 19, 59 and 68 By use of this approach, it is usually recommended that the capsular incision begin 1 cm from the acetabular rim and continue parallel to the labrum, connecting anterolateral and direct anterior or midanterior portals. Some investigators believe that in cases of poor capsular compliance or preoperative stiffness, capsulectomy may be of therapeutic advantage for some patients.19, 20, 21, 22, 23 and 24 Literature predating the advent of THA describes the use of extensive capsulectomy and synovectomy as a potential treatment option for symptomatic hip arthrosis. 22, 23 and 24 With a resurgence of interest in atraumatic and iatrogenic hip instability, though, there has been a renewed focus on restoring capsular tension and integrity. Case reports of subluxation and dislocation after arthroscopic hip surgery further highlight the potential negative impact of capsulotomy without closure in the presence of hyperlaxity or when normal osseous constraints are compromised.25, 26 and 27
In cases where there is concern for subtle capsular laxity or in athletic individuals without preoperative stiffness, capsular closure has the potential to reduce postoperative microinstability and accelerate recovery. It is important to recognize, however, that “capsular repair” may indicate different things for different surgeons. Some create a T-shaped capsulotomy through the zona orbicularis to improve visualization in the peripheral compartment. At the conclusion of the case, some surgeons close the longitudinal part of the T-capsulotomy using a suture shuttling technique while leaving the transverse part open.18 Other techniques avoid transection of the zone orbicularis altogether and use similar shuttling techniques to repair the portal-to-portal crescent-shaped capsulotomy.9 Our preferred technique for routine capsular closure is described later (Fig 1, Fig 2, Fig 3, Fig 4 and Fig 5, Video 1, available at www.arthroscopyjournal.org). To our knowledge, there has only been 1 reported clinical case of a capsular repair in a native hip: Matsuda26 performed an open direct side-to-side suture repair of the anterior capsule on a patient who sustained an acute iatrogenic dislocation after hip arthroscopy. A summary of the evidence for and against routine capsular closure is included in Table 2.
Fig 1. Routine anterosuperior capsulotomy (12 to 3 o’clock) in a right hip for central and peripheral compartment access during hip arthroscopy.
Fig 2. Anterior view of a right hip after routine anterosuperior capsulotomy (12 to 3 o’clock). The arrows denote respective proximal and distal capsuloligamentous flaps for later repair or plication.
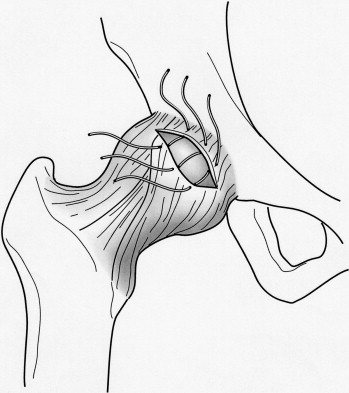
Fig 3. Typical configuration after arthroscopic sutures have been passed in side-to-side fashion between the proximal-to-distal limbs of the respective capsuloligamentous flaps during routine capsular closure.
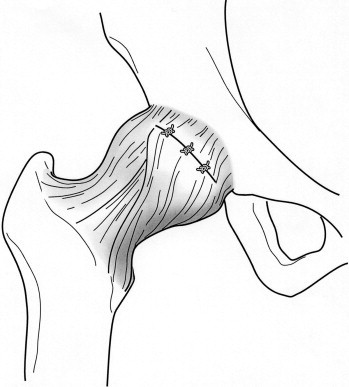
Fig 4. The final repair construct after direct side-to-side capsular closure as viewed from anterior to posterior on a right hip.

Fig 5. The concept of a direct side-to-side capsular repair (arrows) without an inferior shift or capsulorrhaphy.
Table 2. Summary of Evidence for and Against Need for Routine Capsular Closure
| Arguments for Routine Capsular Closure | Arguments Against Routine Capsular Closure |
|
Biomechanical studies support the vital role of an intact hip joint capsule in maintenance of hip stability.2, 3, 4, 8, 20, 32, 33, 34, 35 and 36 |
A systematic review of approximately 4,000 hip arthroscopies for FAI using varying degrees of capsulotomy/capsulectomy (without repair or plication) reported 0 cases of iatrogenic instability.69 |
|
The hip joint capsule has been shown to significantly impact total hip construct stability in both biomechanical and clinical trials.4, 37, 38, 39, 40, 41, 42, 43, 44 and 45 |
Capsulotomy or capsulectomy may have therapeutic advantages in the setting of significant preoperative stiffness or adhesive capsulitis.19, 20, 21 and 22 |
|
Native hip stability is optimized with normal capsular integrity.3 and 8 |
Routine repair/closure in all patients may result in a higher incidence of postoperative stiffness. |
|
Four cases of iatrogenic hip dislocation/subluxation after excessive anterior/lateral rim resection, after bony dysplasia, or in setting of capsular laxity and atraumatic instability have been reported.25, 26, 27 and 70 Postoperative subluxation characterized by an inability to maintain a concentric joint is likely under-reported. |
Atraumatic Instability and Capsulorrhaphy
Atraumatic instability of the hip is a poorly recognized clinical entity that is emerging in the orthopaedic literature as a significant cause of functional impairment in young patients.5, 6, 9 and 71 In a series on revision hip arthroscopy, it was found that 35% of patients with refractory pain after prior arthroscopy had unaddressed instability.10 In some instances, a single insult can lead to capsular and soft-tissue attenuation, which renders the joint prone to further subacute instability events. In most cases, however, atraumatic instability occurs as the result of dynamic overuse or from participation in sports that involve repetitive hip rotation with axial loading (figure skating, dance, gymnastics, baseball, golf, martial arts, and so on). Repetitive stress on the anterior capsular stabilizers can lead to iliofemoral ligament strain and, ultimately, plastic deformity and capsular redundancy.6 This can, in turn, progress on a continuum, to microinstability, anteromedial labral injury, and secondary compensatory changes.49, 60 and 72
Whereas making the diagnosis of atraumatic hip instability is challenging in its own right, treatment of the underlying pathophysiological process is even more challenging. Patients with atraumatic hip instability often exhibit a spectrum of subtle morphologic abnormalities or patterns of connective tissue dysfunction or may even have underlying systemic conditions. Once the diagnosis is suspected clinically and conservative measures have failed, intraoperative findings are useful to confirm the diagnosis. The joint may distract easily, and greater displacement of the femoral head from the acetabulum may be seen. Arthroscopic visualization may show overt laxity or thinning of the capsule. Furthermore, indirect signs of atraumatic instability, such as ligamentum teres tears, are demonstrable intraoperatively. Domb and colleagues73 defined a “stability index” and found that ligamentum tears are more common in hips with a lower lateral center-edge angle and higher inclination, as well as in hips without acetabular retroversion.
The use of open suture capsulorrhaphy for recurrent anterior and posterior hip instability has been reported for decades.6, 49, 50, 51, 52, 54, 55, 56 and 57 Recent technical advances, coupled with an improved understanding of atraumatic hip instability, have allowed the arthroscopic hip surgeon to address some of the contributing soft-tissue influences on this disease spectrum in a much less invasive manner. Arthroscopic capsular tightening may be achieved in a number of ways5, 6, 9, 10, 25, 28, 29, 31, 47, 49, 50, 51, 52, 53, 54, 55, 56 and 57 and can be performed in isolation or in conjunction with other necessary intra-articular work. Our preferred technique is discussed later.
Many of the principles used to perform arthroscopic hip capsulorrhaphy or plication have been adapted from techniques used in shoulder arthroscopy. Satisfactory biological healing has been confirmed histologically and radiographically.74, 75 and 76 Thermal capsulorrhaphy was first reported by Philippon47 and 48 in a series of patients with atraumatic instability and continues to be used with success today.5 and 30 A number of elite professional athletes have returned to high-level competition after thermal capsulorrhaphy for symptomatic hip instability. Al-though thermal necrosis, chondrolysis, and capsular attenuation are well-known complications associated with the use of thermal capsulorrhaphy in the shoulder, these adverse effects have yet to be reported in the hip.77
The setting of hyperlaxity with concomitant intra-articular pathology presents a challenging dilemma to the arthroscopic hip surgeon. When strategic anterosuperior capsulotomy is necessary to facilitate instrument passage and implant placement, suture capsulorrhaphy remains the only major treatment option present in the literature. Techniques to address combined chondral-labral injuries or FAI and capsular laxity have been described.9, 28 and 31 Arthroscopic suture plication or capsulorrhaphy, though technically demanding, has achieved consistent success in small case series and reports.10, 25, 28, 29, 31 and 53 Most technical descriptions recommend that a variable number of sutures should be shuttled with a hooked suture shuttling device and then retrieved with a soft-tissue penetrator. Tension of the plication can be controlled by altering the size of the “bite” incorporated or by penetrating more distally into the capsular expansion at the zona orbicularis when retrieving the passed suture. An inferior shift can also be achieved by carefully modifying the location of tissue gathered in the plication construct. Because the anterior capsuloligamentous complex normally tightens in extension, an inferior shift may potentiate the screw-home mechanism and enhance dynamic tension in this position. Our preferred technique to achieve an inferior capsular shift is described in further detail later. Techniques for posterior and posterosuperior capsular plication have also been described.6 The application of arthroscopic capsular plication has even been expanded to use in well-positioned unstable THA.53 Factors impacting the decision whether to leave the capsulotomy open or perform capsular repair plication are listed in Table 3.
Table 3. Factors That Influence Need for Capsulotomy/Capsulectomy, Capsular Closure, or Capsular Placation
| Findings |
Capsulotomy/Capsulectomy |
Capsular Closure |
Capsular Plication |
|
Clinical |
Preoperative stiffness |
Young athletic patients |
Systemic condition of supraphysiological laxity |
|
Underlying rheumatologic condition requiring extensive synovectomy/capsulectomy |
Female patients without preoperative stiffness |
Clinical examination consistent with capsular incompetence, atraumatic instability, or increased physiological laxity9 |
|
|
Synovial proliferative disorder |
After bariatric surgery |
History of capsular plication of another joint |
|
|
Clinical concern for adhesive capsulitis |
Impaired neuromuscular function or dynamic stability |
Impaired neuromuscular function or dynamic stability |
|
|
Normal neuromuscular function |
|||
|
Radiographic |
Normal anterior and lateral CEA, acetabular index, stability index73 |
Borderline or greater acetabular dysplasia (CEA 20°-24°) or deficiency of bony constraint (acetabular index, stability index) |
Borderline or greater acetabular dysplasia (CEA 20°-24°) or deficiency of bony constraint (acetabular index, stability index) |
|
Limited intraoperative distraction |
Easy distraction with minimal force |
Positive intraoperative vacuum sign |
|
|
Capsular redundancy on MR arthrogram, labral or ligamentum teres hypertrophy78 |
|||
|
Arthroscopic |
Capsular hypertrophy, thickening, or limited compliance on manual probing |
Associated ligamentum teres tears73 |
Capsular redundancy or laxity on manual probing |
|
Hyperemic or injected synovium, synovitis consistent with adhesive capsulitis |
Normal-appearing minimally injected synovium |
Weakened, thin capsule |
|
|
Normal capsular compliance |
Associated ligamentum teres tears or insufficiency |
||
|
Sufficient capsular tissue to permit repair without overtightening |
|||
|
Concern for excessive anterior acetabular rim resection |
CEA, center-edge angle; MR, magnetic resonance. Table options
Authors’ Preferred Technique
Capsulotomy With Routine Closure
An arthroscopic approach is performed in traction in the supine position. Anterolateral and midanterior portals are established using a safe access technique. A capsulotomy is performed with a beaver blade, incising the capsule parallel to the acetabular rim from 12 to 3 o’clock (Fig 1). This results in connection of the capsular entry portals. A central compartment diagnostic arthroscopy is performed, with attention to patterns of injury that may indicate impingement or instability. Heralds of instability may include easy distraction of the joint, a thin capsule, and tearing of the ligamentum teres.79 Intra-articular procedures are performed as indicated, commonly including treatment of labral tears, FAI, and cartilage damage. If a ligamentum teres tear is present, debridement may be performed as described by Byrd and Jones.80
At the conclusion of the intra-articular procedures, closure of the capsulotomy is performed (Fig 2, Fig 3, Fig 4 and Fig 5, Video 1). With the hip in 45° of flexion, a disposable cannula (Arthrex, Naples, FL) is introduced through the midanterior portal. A crescent penetrator (Arthrex) is used to pass a suture lasso through the capsule on the proximal side of the capsulotomy. The bird-beak penetrator is then used to retrieve the lasso through the capsule on the distal side of the capsulotomy near the zona orbicularis (Fig 3). The lasso is used to pass a permanent or absorbable suture, achieving a side-to-side stitch (Fig 4 and Fig 5). This is tied arthroscopically with the knot outside of the capsule. A total of between 2 and 4 side-to-side stitches may be placed to complete the capsular closure. The hip is then brought into extension while the surgeon is watching the capsular closure arthroscopically, to ensure that the capsule has not been overtightened. Some technical pearls for routine capsular closure are listed in Table 4.
Table 4. Technical Pearls for Capsular Closure
| Adequate capsular tissue from the proximal origin adjacent to the acetabulum should be retained. Overzealous ablation or resection may compromise any viable tissue available for later repair or result in an overtensioned repair construct. |
|
Use of a suture lasso with a “wheeled” delivery system can optimize delivery for subsequent retrieval without inadvertent suture lasso removal. |
|
If side-to-side closure is not possible and instability is a concern, a more proximal row of suture anchors can be placed along the rim of the acetabulum and subsequently retrieved from under the distal limb of the capsule and tied in extracapsular fashion. |
|
Frequent dynamic examination can aid in the determination/assessment of adequate tension. |
|
Sutures should always be tied with the joint in a reduced position. |
|
A cannula should be placed just outside the capsule to prevent a “soft-tissue bridge” when performing blind arthroscopic knot tying. |
Capsular Plication for Microinstability
Capsulotomy is performed as just described, followed by diagnostic hip arthroscopy and procedures as indicated for treatment of labral tears, FAI, or other intra-articular pathology. At the conclusion of all intra-articular procedures, capsular plication is performed with the hip in 45° of flexion (Fig 6, Fig 7 and Fig 8, Video 1). Side-to-side stitches are passed by use of the technique for suture passage described earlier for capsular closure. However, the sutures are passed in such a fashion that larger bites of the capsule on the distal side are taken, passing the suture through the zona orbicularis itself. Taking larger bites leads to imbrication of the capsule, increasing the tightness of the capsule in external rotation (Fig 6 and Fig 7). In addition, the location of suture passage through the zona orbicularis is more medial than the corresponding point of passage of the same suture on the proximal side of the capsule (Fig 6 and Fig 7). When the sutures are tied outside of the capsule, this results in an inferior shift. The inferior shift augments the screw-home mechanism of the hip by accentuating the spiral orientation of the capsular fibers (Fig 8). This increases the degree to which the capsule tightens in extension. A total of between 2 and 5 stitches are used. The hip is then brought into extension while the surgeon is watching the capsular closure arthroscopically, to ensure that the capsule has not been overtightened. The combination of imbrication and inferior shift increases the tightness of the capsule in both external rotation and extension and thus diminishes potential anterior instability in that position.
Fig 6. Anterior view of a right hip with arrows indicating the proposed direction of capsuloligamentous shift during arthroscopic capsular plication. Figure options
Fig 7. Typical configuration after arthroscopic sutures have been passed through the capsuloligamentous flaps from distal-inferior to proximal-superior to achieve a superior capsular shift. Figure options
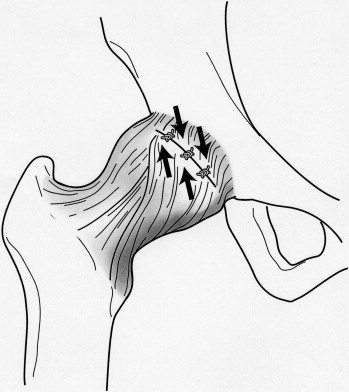
Fig 8. Final capsular plication illustrating re-creation of the natural screw-home mechanism of the native hip capsule.
Figure options
Summary
An exhaustive review of the available literature on the hip joint capsule was carried out to better understand the role of the capsule in maintaining hip joint stability. Our analysis supports the contention that indiscriminate capsulotomy can compromise hip stability but may be beneficial in stiff hip conditions. Biomechanical data strongly favor maintaining or restoring the capsule to an intact state whenever possible to normalize kinematics and reduce the risk of idiopathic instability. Furthermore, clinical data from the hip arthroplasty literature reinforce the importance of capsular repair to maintain postoperative joint construct stability. Although short-term and midterm outcome studies report an overall high rate of success after hip arthroscopy, there remains a considerable subset of patients who do not benefit from surgery or who require early conversion to THA. It is conceivable that a more dedicated approach to maintaining capsular integrity will result in improved outcomes and an even higher long-term success rate. Therefore it is prudent for the arthroscopic hip surgeon to consider routine repair of the capsule (or at least a portion of the capsule) in all cases where stiffness is not a predominant feature. In appropriate circumstances where atraumatic instability or excess capsular laxity is suspected, capsular plication or capsulorrhaphy should be considered. Although the available clinical data on hip capsulorrhaphy are lacking, early and midterm outcomes of open or arthroscopic techniques remain favorable. Whereas arthroscopic cap-sular closure or plication techniques remain technically challenging, it is important that the arthroscopic hip surgeon become facile with these techniques as data supporting the critical role of the capsule continue to emerge.
Conclusions
Biomechanical and clinical studies have consistently shown that the hip joint capsule plays an important role in maintaining stability of the hip joint. Attenuation of the capsule from traumatic, atraumatic, or iatrogenic etiologies may lead to microinstability or macroinstability of the joint. Arthroscopic hip surgeons have traditionally used an unrepaired capsulotomy or capsulectomy with favorable clinical outcomes and without appreciable sequelae. Although in some cases strategic capsulotomy or focal capsulectomy may be therapeutic, injudicious capsulotomy should be avoided at all costs. Furthermore, as the role of the capsule continues to be studied and defined, arthroscopic hip surgeons should become facile with arthroscopic repair or plication techniques to restore proper capsular integrity and tension when indicated.
Supplementary data
Video 1. Sequential arthroscopic suture passage, shuttling, and imbrication technique for arthroscopic capsulorrhaphy of the hip. Help with AVI files Options
References
- M.R. Torry, M.L. Schenker, H.D. Martin et al.
- Neuromuscular hip biomechanics and pathology in the athlete
- Clin Sports Med, 25 (2006), pp. 174-197
- [SD-008]
- C.A. Myers, B.C. Register, P. Lertwanich et al.
- Role of the acetabular labrum and the iliofemoral ligament in hip stability: An in vitro biplane fluoroscopy study
- Am J Sports Med, 39 (2011), pp. 85S-91S (suppl)
- [SD-008]
- J.M. Elkins, N.J. Stroud, M.J. Rudert et al.
- The capsule’s contribution to total hip construct stability—A finite element analysis
- J Orthop Res, 29 (2011), pp. 1642-1648
- [SD-008]
- R.E. Boykin, A.W. Anz, B.D. Bushnell et al.
- Hip instability
- J Am Acad Orthop Surg, 19 (2011), pp. 340-349
- [SD-008]
- M.K. Shindle, A.S. Ranawat, B.T. Kelly
- Diagnosis and management of traumatic and atraumatic hip instability in the athletic patient
- Clin Sports Med, 25 (2006), pp. 309-326
- [SD-008]
- N.V. Bardakos, R.N. Villar
- The ligamentum teres of the adult hip
- J Bone Joint Surg Br, 91 (2009), pp. 8-15
- [SD-008]
- H. Ito, Y. Song, D.P. Lindsey
- The proximal hip joint capsule and the zona orbicularis contribute the hip joint stability in distraction
- J Orthop Res, 27 (2009), pp. 989-995
- [SD-008]
- B. Shu, M.R. Safran
- Hip instability: Anatomic and clinical considerations of traumatic and atraumatic instability
- Clin Sports Med, 30 (2011), pp. 349-367
- [SD-008]
- M.J. Philippon, M.L. Schenker, K.K. Briggs et al.
- Revision hip arthroscopy
- Am J Sports Med, 35 (2007), pp. 1918-1921
- [SD-008]
- J.C. Loh, Y. Fukuda, E. Tsuda, R.J. Steadman, F.H. Fu, S.L. Woo
- Knee stability and graft function following anterior cruciate ligament reconstruction: Comparison between 11 o’clock and 10 o’clock femoral tunnel placement. 2002 Richard O’Connor Award paper
- Arthroscopy, 19 (2003), pp. 297-304
- [SD-008]
- A. Bedi, D.W. Altchek
- The “footprint” anterior cruciate ligament technique: An anatomic approach to anterior cruciate ligament reconstruction
- Arthroscopy, 25 (2009), pp. 1128-1138
- [SD-008]
- J.H. Lubowitz, G.G. Poehling
- Watch your footprint: Anatomic ACL reconstruction
- Arthroscopy, 25 (2009), pp. 1059-1060
- [SD-008]
- R. Ganz, T.J. Gill, E. Gautier et al.
- Surgical dislocation of the adult hip: A technique with full access to the femoral head and acetabulum without the risk of avascular necrosis
- J Bone Joint Surg Br, 83 (2001), pp. 1119-1124
- [SD-008]
- C.M. Larson, M.R. Giveans
- Arthroscopic debridement versus refixation of the acetabular labrum associated with femoroacetabular impingement
- Arthroscopy, 25 (2009), pp. 369-376
- [SD-008]
- R. Ganz, J. Parvizi, M. Beck, M. Leunig, H. Nötzli, K.A. Siebenrock
- Femoroacetabular impingement. A cause for osteoarthritis of the hip
- Clin Orthop Relat Res (2003), pp. 112-120
- [SD-008]
- M.J. Philippon, M.L. Schenker
- Arthroscopy for the treatment of femoroacetabular impingement in the athlete
- Clin Sports Med, 25 (2006), pp. 299-308
- [SD-008]
- C.S. Mauro, J.E. Voos, B.T. Kelly
- Femoroacetabular impingement surgical techniques
- Oper Tech Orthop, 10 (2010), pp. 223-230
- [SD-008]
- M.J. Philippon, A.J. Stubbs, M.L. Schenker et al.
- Arthroscopic management of femoroacetabular impingement: Osteoplasty technique and literature review
- Am J Sports Med, 35 (2007), pp. 1571-1580
- [SD-008]
- H.D. Martin, A. Savage, B.A. Braly, I.J. Palmer, D.P. Beall, B. Kelly
- The function of the hip capsular ligaments: A quantitative report
- Arthroscopy, 24 (2008), pp. 188-195
- [SD-008]
- T.J.W. Byrd, K.S. Jones
- Adhesive capsulitis of the hip
- Arthroscopy, 22 (2006), pp. 89-94
- [SD-008]
- Guilleminet M
- Capsulectomy in the treatment of coxarthritis
- Mem Acad Chir (Paris), 76 (1950), pp. 128-138 (in French)
- [SD-008]
- Guilleminet M
- Good results from capsulectomy of the hip for non-deforming arthrosis
- Lyon Chir, 46 (1951), pp. 237-239 (in French)
- [SD-008]
- L.H. Walton
- Notes on a case of bilateral arthritis of the hip joints treated by capsulectomy
- Proc R Soc Med, 32 (1939), pp. 827-830
- [SD-008]
- A.S. Ranawat, M. McClincy, J.K. Sekiya
- Anterior dislocation of the hip after arthroscopy in a patient with capsular laxity of the hip: A case report
- J Bone Joint Surg Am, 91 (2009), pp. 192-197
- [SD-008]
- D.K. Matsuda
- Acute iatrogenic dislocation following hip impingement arthroscopic surgery
- Arthroscopy, 25 (2009), pp. 400-405
- [SD-008]
- Y. Benali, B.D. Katthagen
- Hip subluxation as a complication of arthroscopic debridement
- Arthroscopy, 25 (2009), pp. 405-407
- [SD-008]
- M.V. Smith, J.K. Sekiya
- Hip instability
- Sports Med Arthrosc, 18 (2010), pp. 108-112
- [SD-008]
- D.M. Epstein, D.J. Rose, M.J. Philippon
- Arthroscopic management of recurrent low energy anterior hip dislocation in a dancer: A case report and review of literature
- Am J Sports Med, 38 (2010), pp. 1250-1254
- [SD-008]
- M.J. Philippon, M.L. Schenker
- Athletic hip injuries and capsular laxity
- Oper Tech Orthop, 15 (2005), pp. 261-266
- [SD-008]
- J.L. Bayer, J.K. Sekiya
- Hip instability and capsular laxity
- Oper Tech Orthop, 20 (2010), pp. 237-241
- [SD-008]
- J. Hewitt, F. Guilak, R. Glisson et al.
- Regional material properties of the human hip joint capsule ligaments
- J Orthop Res, 19 (2001), pp. 359-364
- [SD-008]
- J.D. Hewitt, R.R. Glisson, F. Guilak, T.P. Vail
- The mechanical properties of the human hip capsule ligaments
- J Arthroplasty, 17 (2002), pp. 82-89
- [SD-008]
- K.J. Stewart, R.H. Edmonds-Wilson, R.A. Brand, T.D. Brown
- Spatial distribution of hip capsule structural and material properties
- J Biomech, 35 (2002), pp. 1491-1498
- [SD-008]
- J.J.M. Telleria, D.P. Lindsey, N.J. Giori, M.R. Safran
- An anatomic arthroscopic description of the hip capsular ligaments for the hip arthroscopist
- Arthroscopy, 27 (2011), pp. 628-636
- [SD-008]
- W.M. Mihalko, L.A. Whiteside
- Hip mechanics after posterior structure repair in total hip arthroplasty
- Clin Orthop Relat Res (2004), pp. 194-198
- [SD-008]
- S.J. Tsai, C.T. Wang, C.C. Jiang
- The effect of posterior capsule repair upon post-operative hip dislocation following primary total hip arthroplasty
- BMC Musculoskelet Disord, 9 (2008), pp. 1471-1477
- [SD-008]
- D.J. Chivas, K. Smith, M. Tanzer
- Role of capsular repair on dislocation in revision total hip arthroplasty
- Clin Orthop Relat Res, 453 (2006), pp. 147-152
- [SD-008]
- R.E. White, T.J. Forness, J.K. Allman, D.W. Junick
- Effect of posterior capsular repair on early dislocation in primary total hip replacement
- Clin Orthop Relat Res (2001), pp. 163-167
- [SD-008]
- W.M. Goldstein, T.F. Gleason, M. Kopplin et al.
- Prevalence of dislocation after total hip arthroplasty through a posterolateral approach with partial capsulotomy and capsulorrhaphy
- J Bone Joint Surg Am, 83 (2001), pp. 2-7 (suppl 2)
- [SD-008]
- F.Y. Chiu, C.M. Chen, T.Y. Chung, W.H. Lo, T.H. Chen
- The effect of posterior capsulorrhaphy in primary total hip arthroplasty: A prospective randomized study
- J Arthroplasty, 15 (2000), pp. 194-199
- [SD-008]
- J.M. Van Warmerdam, W.A. McGann, J.R. Donnelly, J. Kim, R.B. Welch
- Achilles allograft reconstruction for recurrent dislocation in total hip arthroplasty
- J Arthroplasty, 26 (2011), pp. 941-948
- [SD-008]
- E.L. Masterson, R. Ferracini, A.M. Griffin, J.S. Wunder, R.S. Bell
- Capsular replacement with synthetic mesh: Effectiveness in preventing postoperative dislocation after wide resection of proximal femoral tumors and prosthetic reconstruction
- J Arthroplasty, 13 (1998), pp. 860-866
- [SD-008]
- S.H. Weeden, W.G. Paprosky, J.W. Bowling
- The early dislocation rate in primary total hip arthroplasty following the posterior approach with posterior soft-tissue repair
- J Arthroplasty, 18 (2003), pp. 709-713
- [SD-008]
- E.R. Henderson, J.M. Jennings, G.A. Marulanda, B.T. Palumbo, D. Cheong, G.D. Letson
- Purse-string capsule repair to reduce proximal femoral arthroplasty dislocation for tumor—A novel technique with results
- J Arthroplasty, 25 (2010), pp. 654-657
- [SD-008]
- M.K. Shindle, J.E. Voos, S.J. Nho et al.
- Arthroscopic management of labral tears in the hip
- J Bone Joint Surg Br, 90 (2008), pp. 2-19
- [SD-008]
- M.J. Philippon
- New frontiers in hip arthroscopy: The role of arthroscopic hip labral repair and capsulorrhaphy in the treatment of hip disorders
- Instr Course Lect, 55 (2006), pp. 309-316
- [SD-008]
- M.J. Philippon
- The role of arthroscopic thermal capsulorrhaphy in the hip
- Clin Sports Med, 20 (2001), pp. 817-829
- [SD-008]
- C. Bellabarba, M.B. Sheinkop, K.N. Kuo
- Idiopathic hip instability. An unrecognized cause of coxa saltans in the adult
- Clin Orthop Relat Res (1998), pp. 261-271
- [SD-008]
- J.R. Lieberman, D.W. Altchek, E.A. Salvati et al.
- Recurrent dislocation of a hip with a labral lesion: Treatment with a modified Bankart-type repair
- J Bone Joint Surg Br, 75 (1993), pp. 1524-1527
- [SD-008]
- P. Birmingham, J. Cluett, B. Shaffer
- Recurrent posterior dislocation of a hip with a Bankart-type lesion: A case report
- Am J Sports Med, 38 (2010), pp. 388-391
- [SD-008]
- B. Graham, R.A. Lapp
- Recurrent posttraumatic dislocation of the hip. A report of two cases and review of the literature
- Clin Orthop Relat Res (1990), pp. 115-119
- [SD-008]
- R. Cuéllar, I. Aguinaga, I. Corcuera, J. Ponte, J. Usabiaga
- Case report: Arthroscopic treatment of unstable total hip replacement
- Arthroscopy, 26 (2010), pp. 861-865
- [SD-008]
- D.A. Stein, D.B. Polatsch, D.J. Rose
- Low-energy anterior hip dislocation in a dancer
- Am J Orthop (Belle Mead NJ), 31 (2002), pp. 591-594
- [SD-008]
- H.J.C. Rashleigh-Belcher, S.R. Cannon
- Recurrent dislocation of the hip with a Bankart-type lesion
- J Bone Joint Surg Br, 68 (1986), pp. 398-399
- [SD-008]
- D. Dall, I. Macnab, A. Gross
- Recurrent anterior dislocation of the hip
- J Bone Joint Surg Br, 52 (1970), pp. 574-576
- [SD-008]
- F. Liebenberg, G.F. Dommisse
- Recurrent post-traumatic dislocation of the hip
- J Bone Joint Surg Br, 51 (1969), pp. 632-637
- [SD-008]
- C.J. Dy, M.T. Thompson, M.T. Crawford et al.
- Tensile strain in the anterior part of the acetabular labrum during provocative maneuvering of the normal hip
- J Bone Joint Surg Am, 90 (2008), pp. 1464-1472
- [SD-008]
- B.T. Kelly, D.E. Weiland, M.L. Schenker, M.J. Philippon
- Arthroscopic labral repair in the hip: Surgical technique and review of the literature
- Arthroscopy, 21 (2005), pp. 1496-1504
- [SD-008]
- J.E. Voos, Cs Mauro, B.T. Kelly
- Femoroacetabular impingement in the athlete: Compensatory injury patterns
- Oper Tech Orthop, 20 (2010), pp. 231-236
- [SD-008]
- M.J. Philippon, K.K. Briggs, Y.M. Yen, D.A. Kuppersmith
- Outcomes following hip arthroscopy for femoroacetabular impingement with associated chondrolabral dysfunction: Minimum two-year follow-up
- J Bone Joint Surg Br, 91 (2009), pp. 16-23
- [SD-008]
- M.J. Philippon, B.G. Souza, K.K. Briggs
- Hip arthroscopy for femoroacetabular impingement in patients aged 50 years and older
- Arthroscopy, 28 (2012), pp. 59-65
- [SD-008]
- J.W. Byrd, K.S. Jones
- Prospective analysis of hip arthroscopy with 10-year followup
- Clin Orthop Relat Res, 468 (2010), pp. 741-746
- [SD-008]
- A.S. Ranawat, B.T. Kelly
- Anatomy of the hip: Open and arthroscopic structure and function
- Oper Tech Orthop, 15 (2005), pp. 160-174
- [SD-008]
- F.K. Fuss, A. Bacher
- New aspects of the morphology and function of the human hip joint ligaments
- Am J Anat, 192 (1991), pp. 1-13
- [SD-008]
- C.O. Lovejoy
- Evolution of human walking
- Sci Am, 259 (1988), pp. 82-89
- [SD-008]
- S. Thorpe
- Origin of human bipedalism as an adaptation for locomotion on flexible branches
- Science, 316 (2007), pp. 1328-1331
- [SD-008]
- T.J.W. Byrd, K.S. Jones
- Arthroscopic management of femoroacetabular impingement in athletes
- Am J Sports Med, 39 (2011), pp. 7S-13S (suppl)
- [SD-008]
- V.M. Ilizaliturri
- Complications of arthroscopic femoroacetabular impingement treatment: A review
- Clin Orthop Relat Res, 467 (2009), pp. 760-768
- [SD-008]
- B.G. Souza, W.S. Dani, E.K. Honda et al.
- Do complications in hip arthroscopy change with experience?
- Arthroscopy, 26 (2010), pp. 1053-1057
- [SD-008]
- C.M. Blakey, M.H. Field, P.J. Singh, R. Tayar, R.E. Field
- Secondary capsular laxity of the hip
- Hip Int, 20 (2010), pp. 497-504
- [SD-008]
- C.M. Powers
- The influence of abnormal hip mechanics on knee injury: A biomechanical perspective
- J Orthop Sports Phys Ther, 40 (2010), pp. 42-51
- [SD-008]
- I.B. Botser, D.E. Martin, B.G. Domb
- Relationship between tears of the ligamentum teres and acetabular undercoverage: Does microinstability play a role?
- Proceedings at the (2011) International Society of Hip Arthroscopy Meeting, Paris, France, September 2011
- [SD-008]
- B.T. Kelly, A.S. Turner, M. Bansal et al.
- In vivo healing after capsular plication in an ovine shoulder model
- Iowa Orthop J, 25 (2005), pp. 95-101
- [SD-008]
- P.M. Pellicci, H.G. Potter, L.F. Foo, F. Boettner
- MRI shows biologic restoration of posterior soft tissue repairs after THA
- Clin Orthop Relat Res, 467 (2009), pp. 940-945
- [SD-008]
- E.P. Su, C.R. Mahoney, R.S. Adler, D.E. Padgett, P.M. Pellicci
- Integrity of repaired posterior structures after THA
- Clin Orthop Relat Res, 447 (2006), pp. 43-47
- [SD-008]
- K.L. Wong, G.R. Williams
- Complications of thermal capsulorrhaphy of the shoulder
- J Bone Joint Surg Br, 83 (2001), pp. 151-155
- [SD-008]
- D.R. Armfield, J.D. Towers, D.D. Robertson
- Radiographic and MR imaging of the athletic hip
- Clin Sports Med, 25 (2006), pp. 211-239
- [SD-008]
- I.B. Botser, D.E. Martin, B.G. Domb
- Tears of the ligamentum teres: Prevalence in hip arthroscopy using two classification systems
- Am J Sports Med, 39 (2011), pp. 117S-125S (suppl)
- [SD-008]
- J.W. Byrd, K.S. Jones
- Traumatic rupture of the ligamentum teres as a source of hip pain
- Arthroscopy, 32 (2004), pp. 385-391
- [SD-008]
The authors report the following potential conflict of interest or source of funding in relation to this article: Smith & Nephew.
Address correspondence to Benjamin G. Domb, M.D., Hinsdale Orthopaedics, 550 W Ogden Ave, Hinsdale, IL 60521, U.S.A.